Nuclear deaths from testing
The deaths caused by American nuclear testing were not, for the most part, deaths in the cinematic sense: there was no city flattened, no single morning when thousands of civilians were seen to fall. The toll was slower, quieter and more difficult to count. It came through milk bottles, desert dust, rainwater, fish, bone marrow, thyroid glands and cancers diagnosed decades after the flash had vanished. That is what makes the subject so unsettling. The explosions lasted seconds; the biological aftermath lasted lifetimes.
Between 1945 and 1992, the United States carried out more nuclear test explosions than any other country: more than a thousand in total. The first was Trinity in New Mexico on July 16, 1945; the last was Divider in Nevada on September 23, 1992. The tests took place in New Mexico, Nevada, the Pacific, Alaska, Colorado, Mississippi and elsewhere, but the two great theatres of exposure were the Nevada Test Site and the Marshall Islands.
The most cautious official estimates usually begin with the American population exposed to fallout from tests at the Nevada Test Site and from worldwide atmospheric testing. One major estimate projected about 11,000 extra cancer deaths in the United States from external exposure to fallout among people alive at any time from 1951 to 2000, with about 22,000 total cancer cases when nonfatal cancers are included. It also estimated that about 1,100 of those deaths would be from leukemia, with additional leukemia cases from internal exposure to bone-seeking radionuclides such as strontium-90.
That 11,000 figure is not the whole story. It is best understood as a conservative, model-based estimate for one major pathway of harm: external radiation exposure from fallout. Broader estimates that include other exposure pathways have put the likely toll at roughly 17,000 cancer deaths and about 80,000 cancer cases in the United States from atmospheric nuclear-testing fallout. These estimates include thyroid-cancer deaths, leukemia deaths from internal exposure, deaths from external exposure, and additional deaths from internal exposure to radionuclides such as carbon-14, tritium and cesium-137.
The reason the numbers vary so widely is that fallout did not behave like a neat poison dropped into a single well. It moved with wind, rain, food chains and human habits. A ranch child drinking fresh goat’s milk in Utah could receive a far higher thyroid dose than an adult in a city drinking commercially mixed milk. A storm could wash radionuclides onto one county and spare the next. A bomb detonated from a tower or near the ground sucked soil and debris into the fireball, made those particles radioactive, and then scattered them as fallout. Some particles were heavy and fell nearby; others rose high into the atmosphere and travelled across continents.
The most infamous isotope in the American downwinder story is iodine-131. It has a short half-life of about eight days, which sounds reassuring until one realizes that it enters the body quickly. Cows and goats ate contaminated pasture. Their milk carried iodine-131. Children drank the milk. The thyroid gland, especially in children, eagerly absorbed iodine because it needs iodine to make hormones. Once lodged in the thyroid, iodine-131 irradiated a small organ at close range.
This is why the nuclear-testing death toll is so hard to imagine. A bomb exploded in Nevada; a child hundreds or thousands of miles away drank milk; thirty years later a doctor found a thyroid tumour. The line between those events is scientifically plausible, but individually almost impossible to prove. Epidemiology works in populations, not in certainties for one person. A particular cancer may have happened anyway. Across millions of people, however, small added risks become thousands of illnesses.
Leukemia followed a different biological path. Fallout contained radionuclides that could irradiate bone marrow, where blood cells are made. Strontium-90 was especially feared because the body treats it chemically like calcium, allowing it to enter bones. Bone marrow is sensitive to radiation, and leukemia is one of the cancers most strongly associated with ionizing radiation. Solid cancers could arise through other routes: external gamma radiation passing through the body, inhaled particles lodging in lung tissue, ingested cesium-137 dispersing through soft tissue, or longer-lived radionuclides remaining in soil and food chains.
The Nevada Test Site created a particular kind of American victim: the downwinder. These were people in Nevada, Utah, Arizona, New Mexico and beyond who did not work in nuclear weapons labs and did not volunteer for experiments, but lived under the invisible weather of the Cold War. Many saw the flashes. Some remembered dust on cars, strange tastes in the air, animals sickening, and official reassurances that there was no danger. The official maps and models came much later.
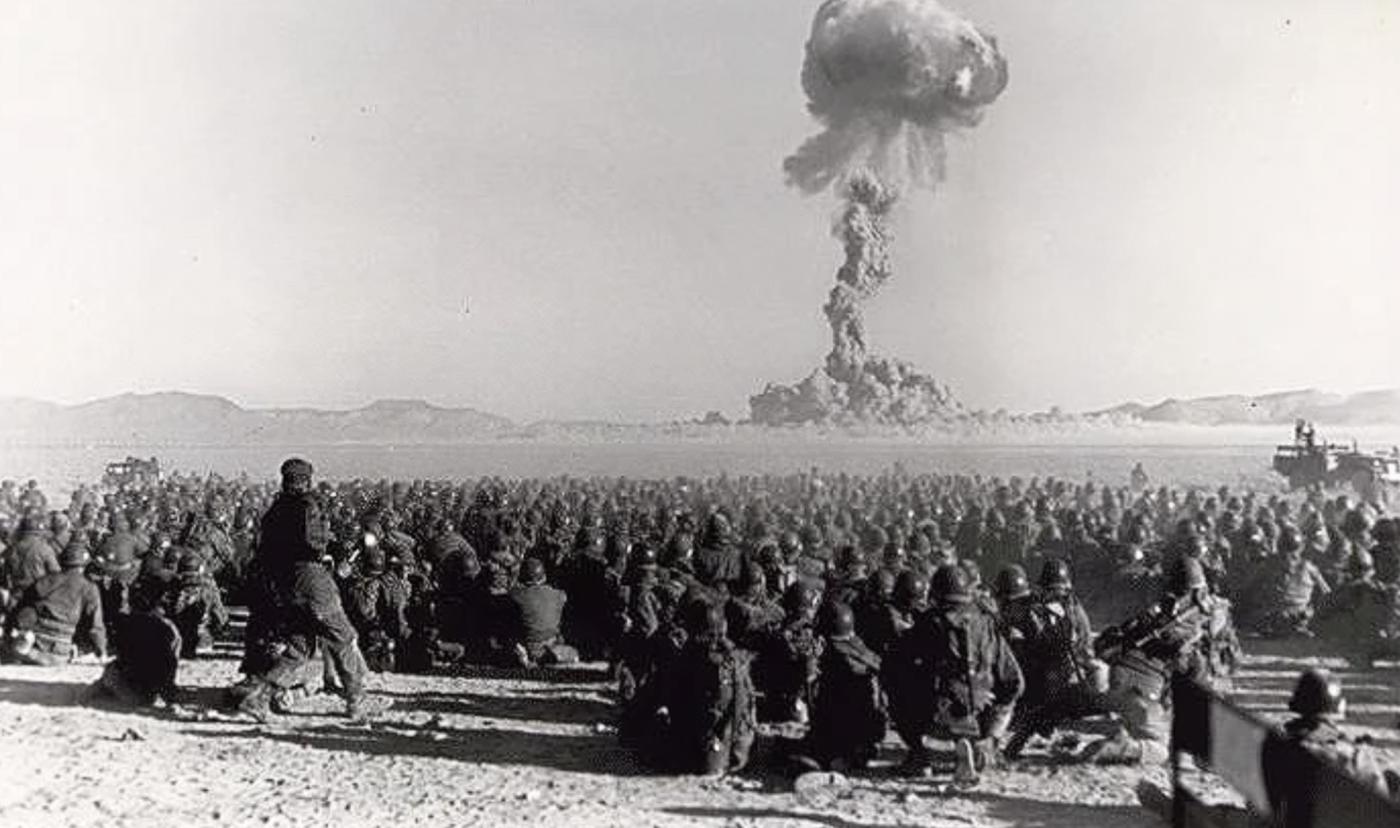
Military personnel were also placed in harm’s way. During the 1950s, soldiers were used in exercises near nuclear detonations to test battlefield behaviour in an atomic war. Some watched blasts from trenches, marched across contaminated ground, or worked on ships and aircraft used in tests. Their exposures varied greatly, and many later illnesses were handled through veteran and compensation systems rather than through a single national death count. The human difficulty is that the same disease categories that appear after radiation exposure, such as leukemia, lung cancer or thyroid cancer, also occur naturally or from smoking, occupational exposure and ordinary ageing.
The Marshall Islands show the problem in a sharper, more intimate form. Between 1946 and 1958, the United States tested nuclear weapons at Bikini and Enewetak. These were not just technical experiments; they were explosions in and around a living oceanic society. The most notorious was Castle Bravo on March 1, 1954. It was expected to be powerful; it was far more powerful than expected. Radioactive coral dust fell on inhabited atolls and on the Japanese fishing boat Daigo Fukuryū Maru, or Lucky Dragon No. 5. Crew members developed acute radiation symptoms; the radio operator, Aikichi Kuboyama, died later in 1954, commonly remembered as the first fatality associated with the hydrogen bomb test.
For Marshallese communities, the harm included acute exposure, displacement, contaminated food, contaminated land, and the slow dread of cancers and thyroid disease. One later estimate projected about 170 excess radiation-related cancers among more than 25,000 Marshallese alive during the relevant period, against a much larger background of cancers expected for other reasons. That sounds numerically small until one looks at the local distribution: for the people on Rongelap, more than half of all cancers were estimated to be attributable to fallout; for Utrik, the proportion was lower but still significant. In small communities, percentages like that do not feel statistical. They feel like relatives, neighbours and family histories.
The illnesses were not limited to cancer. High fallout exposures could cause nausea, vomiting, skin burns, hair loss, immune damage and thyroid abnormalities. Lower exposures were more likely to appear years later as cancer risk. Thyroid nodules, some benign and some malignant, became part of the medical legacy. Psychological harm also mattered: communities were moved, returned, moved again, studied, compensated, argued over and left with landscapes where food, memory and danger became inseparable.
The United States eventually acknowledged enough harm to create compensation systems. The Radiation Exposure Compensation Act, first enacted in 1990, offered payments to certain downwinders, onsite test participants and uranium workers who developed specified diseases. Compensation, however, is not the same as a full death count. Eligibility rules drew lines around geography, dates and diseases. Many people who believed they were harmed fell outside those lines.
A fair estimate, then, depends on what is being counted. For deaths among Americans from U.S. nuclear-testing fallout, a cautious government-based figure is about 11,000 excess cancer deaths from external fallout exposure, while broader estimates that include thyroid cancer and internal exposures rise to around 17,000 deaths and roughly 80,000 cancers. For Marshall Islanders, one major projection estimated about 170 excess cancers, with very high attributable fractions in the most exposed atolls, though not all of those cancers would necessarily be fatal. For directly exposed individuals such as the Lucky Dragon crew, there were acute illnesses and at least one famous death linked to Castle Bravo fallout.
The deepest moral problem is that the dead cannot be counted like battlefield casualties. Nuclear testing converted risk into a national atmosphere. It spread tiny increments of danger across huge populations, while delivering intense doses to unlucky communities under particular plumes. Most victims did not know when they were exposed. Many were children. Many were told they were safe. Some died of cancers that looked ordinary on a death certificate but belonged, statistically, to the bomb.
The American nuclear-testing programme was designed to prove that weapons worked. It also proved something else: that a nuclear explosion does not end when the mushroom cloud loses its shape. It continues as iodine in milk, strontium in bone, cesium in soil, fear in families, and arguments over numbers long after the officials, generals and scientists have left the test site. The most defensible answer is that U.S. nuclear testing probably caused many thousands of deaths and tens of thousands of illnesses, with the best-known estimates ranging from roughly 11,000 to 17,000 excess cancer deaths in the United States alone, depending on which exposure pathways are included. The uncertainty should not be mistaken for innocence. In this case, uncertainty is part of the injury.









